Tapping into controversial back surgeries
Back pain is one of the most common reasons Americans go to the doctor, and one of the fastest growing treatments is spinal fusion surgery. From 2001 to 2011, the number of spinal fusions in U.S. hospitals increased 70 percent, making them more frequently performed than even hip replacements. The growth has been attributed in part to improved technology, an aging population, and a greater demand among older people for mobility. But it has also sparked a debate over whether some surgeons are performing spinal fusions that are unnecessary and potentially dangerous. The procedure fuses together two or more vertebrae often with metal rods and screws, and can result in paralysis or life-threatening complications.

For this six month investigation, CBS News exclusively obtained part of a government database. We asked for, among other things, the number of spinal fusions each doctor in the country billed to Medicare from 2011-2012, under codes most commonly used for "degenerative" conditions that cause lower back pain. We put the entire database online and made it easily searchable by the public. We also provided guidance on how to interpret it and details about how it was compiled.
It is important to note that the data does not reveal whether any of the surgeries that a doctor performed were inappropriate, and includes many spinal fusions that are widely considered necessary. Still, experts say high numbers raise questions and serve as starting points for further investigation. We looked into some of the highest volume surgeons and found some were respected with unblemished records. Others were banned or suspended from hospitals or settled lawsuits alleging unnecessary procedures. All of them are still operating.
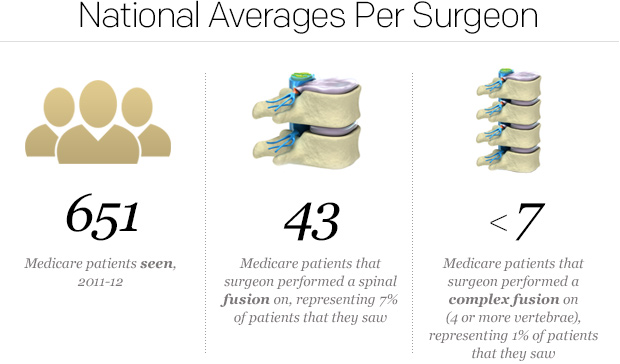
The data shows that a small group of doctors performed these procedures far more frequently than their peers. While the national average was 46 surgeries over the two year period, some did more than 460. While the average spine surgeon performed them on 7 percent of patients they saw, some did so on 35 percent. (Averages exclude doctors that performed 10 or fewer of these fusions. Medicare redacted those figures to protect patient privacy.)
There are multiple reasons why a surgeon may be performing a disproportionate number of fusions. Some may receive lots of referrals and treat more complicated cases. Others may believe the procedure is appropriate for patients that many doctors would not operate on. There is also a financial incentive to performing a spinal fusion. It can earn a surgeon thousands of dollars - and five times as much as less risky alternatives.
Some of the biggest concerns surround more complex fusions that join four or more vertebrae. The more vertebrae that a surgeon fuses, the more they are paid (all else being equal), but the risks increase for the patient as well. One study of complex fusions for stenosis (a narrowing of the spinal canal) found 1 in 20 led to life-threatening complications. When it came to these riskier surgeries, the discrepancy in the data was even larger. Some doctors performed more than 100, while the national average was less than 7. Overall, 5 percent of the surgeons did about 40 percent of the fusions on four or more vertebrae.
We shared these statistics with Dr. Daniel Resnick, Vice Chair of Neurosurgery at the University of Wisconsin School of Medicine and President of the Congress of Neurological Surgeons. He said they raise serious concerns, and suggest that while the majority of spine surgeons are careful about recommending fusions, some may be "operating outside of the generally agreed upon (based on common practice and literature supported guidelines) parameters."
Dr. Resnick added that Medicare, medical societies, and credentialing boards should use data like this to follow practice patterns and patient outcomes. He said surgeons with the highest numbers should be looked at closely and asked to explain themselves.
OVERVIEW | LOOK UP A SURGEON | SURGEONS WE LOOKED INTO | RESPONSE TO OUR FINDINGS
Look up a Surgeon
This database allows you to find and compare spinal fusion operating rates of surgeons nationwide. To start, enter a doctor's last name in UPPER CASE. If the number of patients that they operated on comes up blank, it was between 1 and 10 (Medicare redacted those counts to protect patient privacy). You can also download this spreadsheet with more detailed information. It can be sorted by total fusions and filtered by city or state.
The data includes procedures performed on Medicare patients from 2011-2012. Some of the country's highest volume surgeons discounted its value. They questioned the validity of the numbers and told us (for reasons listed below) that the data should not be used to compare them with their peers. Other doctors said it could be hugely beneficial to patients.
Dr. Sohail Mirza, Chair of Orthopaedics at Dartmouth-Hitchcock Medical Center, said if your surgeon performed significantly more of these fusions than others in your community, or did them on a far higher percentage of their patients, you should ask them why. You may also want to get another opinion. It could just mean they have a sizeable referral base because they are respected in the field, but it could also mean that they are doing surgeries that others would not consider appropriate.
How this database was compiled
We asked Medicare for details on the billing codes for spine surgery and the agency referred us to the American Medical Association, which forwarded us to the North American Spine Society (NASS). One of NASS's billing experts helped us identify the codes most commonly used for spinal fusions that treat degenerative conditions that cause lower back pain. Experts told us to focus on this subset of fusions because it is more controversial, and there is a debate over whether some of them are necessary.
NASS's expert then helped us develop a methodology for counting these surgeries. Specifically, any time CPT code 22558, 22585, 22586, 22612, 22614, 22630, 22632, 22633, or 22634 was billed, it was counted as one spinal fusion surgery. If multiple codes were billed on the same procedure, it was still counted as one surgery. When fusing more than two vertebrae, there are separate "add-on" codes to be billed once per additional vertebra, according to NASS. Any time CPT code 22585, 22614, 22632, or 22634 was duplicated (billed twice) on the same procedure, it was counted as a fusion on four or more vertebrae.
We did not count surgeries where the physician was described as an assistant or team surgeon, or didn't finish the procedure, by excluding codes with modifiers 53, 55, 66, 73, 74, 80, 81, 82, AK, or AS. Doctors that did not have the specialty codes for neurosurgeons, orthopedic surgeons, or physical rehabilitation specialists were also removed from the dataset.
We sent the instructions to the Centers for Medicare and Medicaid Services (CMS). Michael Marquis, Christopher Powers, and Stephanie Bartee at CMS compiled a large spreadsheet with roughly 192,000 fusions by 6,000 doctors. It was the first time Medicare had released spinal fusion data and allowed the names of surgeons to be made public. No patient information was disclosed, and as stated above, counts between 1 and 10 were redacted to protect patient privacy. National averages were calculated among doctors that performed more than 10 total fusions. Fusions on beneficiaries in Medicare's Part C program were not included as those plans are run by private insurers.
Limitations to the data
- The billing codes used to compile this database describe a technique - not a diagnosis. According to NASS, they are most commonly used for treating degenerative conditions, but may also be used for other purposes.
- The billing codes do not indicate whether a fusion was inappropriate, and some widely accepted fusions (like those for spondylolisthesis, or a slipped disc) are billed for using these codes.
- Billing can be confusing and there may be inconsistencies among surgeons in terms of the codes they use for fusions. There may also be billing errors.
- Some surgeons may get more referrals, see more complicated cases and do more fusions as a result. These numbers do not take into account the severity of the conditions the surgeon is treating.
- Since this just covers Medicare patients, physicians in areas with large elderly populations have higher numbers.
- Some of these fusions may include the mid-back or neck, as some of the codes used extend up to that area.
- Some surgeons often perform "360 degree" fusions, which involve two surgeries (through the front and back). Their total number of fusions may be higher as a result, but the number of patients that they fused is not changed by this.
- Some spine surgeons operate on other parts of the body as well. They may have lower numbers and bring down averages.
- Residents, physician assistants, and others under a surgeon's supervision can file claims under that doctor's name. While this is not done for spinal fusion surgeries, it may artificially increase the number of patients that a doctor saw in the data.
- To calculate averages for fusions on four or more vertebrae, we used 10 for each doctor with a redacted count. This was done to avoid overstating the differences between doctors performing many of these fusions and their peers.
- As with all large datasets, there may be miscellaneous errors.
Incorrect address?
If you are a surgeon and your state (or full address in the spreadsheet) is incorrect, check the information you provided to the National Provider Identifier registry. If you have recently changed it, email us at spinesurgeons@cbsnews.com and we will update your information in the database.
OVERVIEW | LOOK UP A SURGEON | SURGEONS WE LOOKED INTO | RESPONSE TO OUR FINDINGS
Surgeons we looked into
Barbara Jo Smith has lived in Clarksville, Tennessee for her whole life. She grew up on a farm, riding horses and chasing her two brothers around. In 1999, she married her childhood sweetheart.
By age 45, Smith had developed debilitating back pain. She saw a chiropractor and a physical therapist, but neither seemed to help. So she went to Nashville spine surgeon Dr. David McCord.

Dr. McCord recommended two spinal fusion surgeries for Barbara Jo Smith, two days apart. In May of 2010 he operated on her, using plates and screws to join three of her vertebrae. Five months later, she says her pain had only worsened. So she went back to Dr. McCord and he performed another spinal fusion.
Today, Barbara Jo Smith says her pain is "a hundred times worse" than before the surgeries, and that she has nerve problems she did not have before. "One foot feels like it's burning, the other feels like it's on ice," she says. "I'm 49 years old and I can't lift anything without dying."
There are always risks with surgery and a bad outcome is not necessarily the doctor's fault. But if an operation wasn't needed to begin with, it's a different story. When it comes to individual cases, surgeons can disagree about whether a spinal fusion is appropriate. So we asked two doctors to tell us, without commenting on Smith's case in particular, whether they generally recommend the procedure for the diagnosis she was given. Both said they do not.
Dr. Daniel Resnick, Vice Chair of Neurosurgery at the University of Wisconsin School of Medicine and President of the Congress of Neurological Surgeons, helps shape national guidelines for spine surgery. Dr. Sohail Mirza, Chair of Orthopaedics at Dartmouth-Hitchcock Medical Center, has published studies on spine surgery and what he considers the overtreatment of back pain. Both doctors said they generally recommend more conservative treatments for patients with Smith's diagnosis.
According to the Medicare database, Dr. McCord performed fusions on 96 patients from 2011-2012. He did them on 34 percent of patients he saw, almost the highest rate in the entire country. And he performed three or more of these surgeries on 20 different patients over that period - the most of any surgeon nationwide.
The number of patients that Dr. McCord has repeatedly operated on may be higher in part because he often performs "360 degree" fusions (as he did on Barbara Jo Smith). The technique involves two surgeries, through the front and back. But other doctors also use this method, and the 20 patients that Dr. McCord operated on three or more times was twice as many patients as any other surgeon nationwide, according to the Medicare database.
In 2012, Dr. McCord was banned from operating at Centennial Medical Center. A confidential report by the hospital reveals that a "hearing committee found that [Dr. McCord] had a pattern of performing spine surgeries on patients for whom surgery is not indicated." Internal and external reviews concluded that he was performing unnecessary hardware removal operations. Dr. McCord sued the hospital, accusing it of conducting a sham review process led by a surgeon that saw him as competition. The case was dismissed.
Dr. McCord's attorney says he will appeal. But it wasn't the first time his surgeries had come under scrutiny at Centennial. CBS News has learned that after a separate review in the late 1990s, Dr. McCord agreed to limit his number of surgeries and get second opinions before operating. He is still practicing at another hospital just blocks away.
Dr. McCord invited CBS News to his office but declined repeated requests for an on-camera interview. He introduced us to three patients and each spoke about how he dramatically improved their lives. In an email, his attorney wrote: "we will not verify many of the[se] misstatements and ill-founded allegations...of the hundreds of patients Dr. McCord has treated, the vast majority of them are much improved."
The lawyer also said Dr. McCord has not settled or lost a malpractice lawsuit, and highlighted Dr. McCord's degrees from top universities. He said Dr. McCord was banned from Centennial because as an orthopedist, the neurosurgeons there did not like him (both specialties perform spine surgery).

"Dr. Jimenez is well aware of and shares the general concern about unnecessary spinal surgeries," a statement reads. "Before a fusion is considered, he treats his patients conservatively with a course of care that might include NSAIDs, physical therapy and injections."
The attorney also objected to the use of billing codes to count spinal fusions for "degenerative" conditions that cause lower back pain. "It is simply not possible to discern the diagnosis(es) from the CPT code alone," she wrote.
It is true that the billing codes describe a technique - not a diagnosis. Some widely accepted fusions are billed for using these same codes. But while the data does not reveal whether any of the fusions that a doctor performed were inappropriate, experts say high numbers raise questions and serve as starting points for further investigation.
When we looked into Dr. Jimenez, we found that in 2006 he was suspended indefinitely by a network of five hospitals in Georgia. According to a confidential report obtained by CBS News, it concluded that he "pose[d] a threat to the life, health and safety of patients." There were concerns about, among other things, his "surgical competency and selection of procedures." Dr. Jimenez eventually left the hospital system and sued it for racial discrimination. He claimed the review committee made up lies to oust him and did not give him a hearing. The case was eventually dismissed.
Dr. Jimenez also settled two malpractice suits in Georgia, for $950,000 in 2006 and $375,000 in 2010, according to the state's medical board. One of the cases was brought by James McCall, a 44-year-old man with back and leg pain, McCall's attorney said. After Dr. Jimenez performed a fusion on three of his vertebrae, McCall suffered permanent nerve damage in his right leg, the complaint says. He could no longer lift his foot and would trip when walking, and his back and leg pain also remained. Dr. Jimenez denied wrongdoing.
We mentioned the hospital suspension and malpractice settlements to the attorney representing Dr. Jimenez, but she chose not to comment on them.

Some of the biggest concerns surround more complex fusions, on four or more vertebrae. A 2010 study in the Journal of the American Medical Association looked at complex fusions for lower back stenosis (a narrowing of the spinal canal) and found 1 in 20 led to life-threatening complications. The Medicare database indicates Dr. Mathew Alexander of Corpus Christi, Texas performed 97 fusion surgeries on four or more vertebrae - the sixth most in the country.
One of Dr. Alexander's patients, a 63-year-old hairdresser named Kimberly Keith, had pain in parts of her head, neck, and left arm. She tried physical therapy and a steroid injection, but neither helped. So in 2010, Dr. Alexander performed a spinal fusion from her skull through six of her vertebrae. The operation took five hours and in a deposition, Dr. Alexander said he had one or two other procedures earlier that day. Keith was billed more than $56,000 in surgical fees, but Dr. Alexander said they likely collected about a third of that amount.
Keith is now suing Dr. Alexander for allegedly aligning her neck crookedly and performing a more aggressive surgery than necessary. She has virtually no movement of her head, and it is stuck in a tilted position looking down and off to the right. Multiple doctors have said a corrective surgery would involve removing rods and screws that Dr. Alexander put in and entail significant risk. The case is ongoing.

Dr. Alexander also said an imperfectly aligned neck is a risk of the surgery that cannot always be avoided. "There's no way you can hundred percent put a patient in neutral position...that's the best we can do for this type of operation."
In the deposition, Keith's attorney pressed Dr. Alexander on why he believed she had severe stenosis (a narrowing of the spinal canal) when multiple radiologists considered it mild or moderate. Dr. Alexander said he disagreed with their readings of the images. "I rely on the radiologist," he said. "But also as a neurosurgeon, we interpret the films, too."
Keith's attorney also asked why he fused the second, third, and fourth vertebrae in her neck, when none of the radiologists mentioned problems in that area. He said that when fusing two separate parts of the spine, it is common practice to include the vertebrae between them. "You have to incorporate the whole thing," he said, or she would "require further surgery down the road."
The Medicare data indicates that Dr. Richard Hynes of Melbourne, Florida performed 107 fusions on four or more vertebrae--the third most in the country. In 2006, a private health insurer dropped him and The B.A.C.K. Center (of which he is president) from its coverage network. "They say we're too aggressive, too expensive," he reportedly told a newspaper at the time. "Medical technology is expensive."

In 2008, Dr. Hynes was sued for allegedly performing an unnecessary spinal fusion. After the operation, his 32-year-old patient developed an infection and required another spinal fusion, medical records show. According to her legal complaint, one of the surgeries damaged her intestine, forcing her to have part of it removed. Dr. Hynes settled the case, but denied wrongdoing.
According to the Florida Office of Insurance Regulation, five payments totaling more than $500,000 were made to former patients of Dr. Hynes by his insurance company from 2005-2012. Three of the cases challenged the necessity of spinal procedures performed by Dr. Hynes.
Through an attorney, Dr. Hynes declined our interview requests for this story. Even after we shared our specific findings, he chose not to respond. His lawyer only suggested we review a separate anti-trust lawsuit filed against Health First, the parent company of the insurer that dropped him from its network.
That case was filed by several physicians and group practices (not including Dr. Hynes). It alleges that the company has a near monopoly on healthcare services in the area, and intimidates doctors or obstructs their ability to practice medicine if they do not refer patients exclusively to its facilities. Health First has denied the allegations.
OVERVIEW | LOOK UP A SURGEON | SURGEONS WE LOOKED INTO | RESPONSE TO OUR FINDINGS
Response to Our Findings
We shared our findings with Dr. Daniel Resnick, Vice Chair of Neurosurgery at the University of Wisconsin School of Medicine and President of the Congress of Neurological Surgeons. He spoke on behalf of himself, not the organizations he is affiliated with.
Dr. Resnick said our findings concerned him. He said they suggest that while most doctors are careful about recommending a fusion, some may be "operating outside of the generally agreed upon (based on common practice and literature supported guidelines) parameters." He added that data on reoperation rates and complication rates should also be made public. That information is "critical to make any value judgments regarding the frequency of procedures performed," he said.
Dr. Resnick added that Medicare, medical societies, and credentialing bodies (including state medical boards and the American Board of Medical Specialties) should use databases like the one in this story to follow practice patterns and patient outcomes. He said surgeons with the highest numbers should be closely looked at and asked to explain themselves. But he said that won't happen without a source of funding, as the work is time consuming and entails legal risk.
Dr. Resnick also emphasized that there are many cases where spinal fusions are clearly necessary. The procedure is widely accepted for treating major spinal deformities (like scoliosis), fractures, tumors, infections, and spondylolisthesis (slipped disc) in the lower back. But some of the nation's top spine surgeons say they rarely perform it for simple back pain, degenerated discs (or "degenerative disc disease"), stenosis (a narrowing of the spinal canal), or a herniated disc.
More than 480,000 spinal fusions are performed in U.S hospitals each year, making them more common than even hip replacements. The annual cost of these surgeries is more than $12 billion, according to the Agency for Healthcare Research and Quality. Experts disagree about how many may be unnecessary, but Dr. Richard Deyo, a critic of the procedure and professor at Oregon Health and Science University believes it could be as much as half. For Medicare and Medicaid patients, taxpayers foot the bill.
OVERVIEW | LOOK UP A SURGEON | SURGEONS WE LOOKED INTO | RESPONSE TO OUR FINDINGS